Scientific revolutions often reveal more about human nature than the technologies themselves. Some of the most transformative technologies of our era do not solve human problems by making us stronger or smarter; they solve them by reducing the effort required to achieve desired outcomes. GLP-1 drugs diminish the biological drive to overeat, while large language models increasingly reduce the cognitive effort required to produce knowledge work. Examining them together reveals surprising parallels in how technology alters human agency.
In the history of science, transformative advances often emerge not from overwhelming conceptual complexity, but from deceptively simple ideas. The discovery that a gut hormone could recalibrate appetite and metabolism has reshaped modern medicine. Likewise, the realisation that statistically predicting the next word in a sequence at sufficient scale could produce systems capable of reasoning-like behaviour has altered the trajectory of computing, education, and knowledge work.
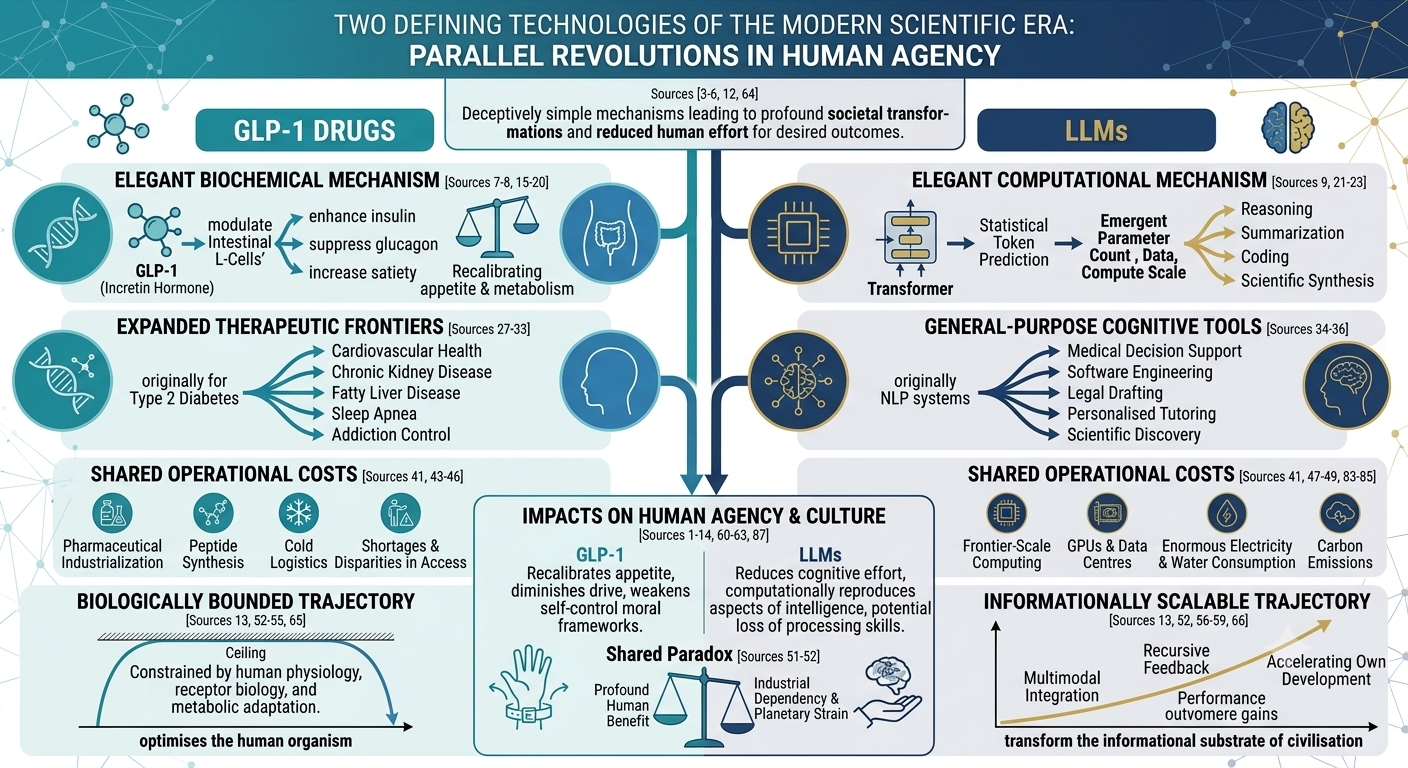
Glucagon-like peptide-1 (GLP-1) receptor agonists and large language models (LLMs) may appear unrelated, one biochemical, the other computational, yet they represent parallel technological revolutions. Both exploit elegant underlying mechanisms that have been studied for decades. Both generate effects far beyond their initial intended use. Both impose substantial environmental and infrastructural costs. Interestingly, they both lead to a loss of agency – one helps us lose weight without all that difficult dieting and the other helps us work without thinking. Despite their shared elegance of design, their futures diverge profoundly: GLP-1 therapeutics remain constrained by biology, while LLMs may represent an effectively unbounded cognitive infrastructure driving the future of civilisation itself.
The comparison is not merely rhetorical. It reveals how modern science increasingly advances through scalable systems capable of amplifying small mechanistic insights into society-wide transformations.
At the core of GLP-1 therapeutics lies a remarkably simple physiological principle. GLP-1 is an incretin hormone secreted from intestinal L-cells after food intake. Its biological role is straightforward: enhance insulin secretion, suppress glucagon release, slow gastric emptying, and increase satiety [1][2]. Pharmacological amplification of this signalling pathway through receptor agonists such as semaglutide and tirzepatide produces dramatic effects on body weight, glycaemic control, and cardiovascular risk [3].
The elegance of the mechanism is striking. Rather than forcing metabolic change through brute biochemical intervention, GLP-1 drugs supraphysiologically modulate endogenous signalling systems already evolved for energy regulation. A relatively narrow receptor pathway produces systemic consequences across appetite, inflammation, vascular biology, and behaviour [1].
LLMs emerged through an analogous conceptual simplicity. Transformer architectures fundamentally operate by predicting the statistically most likely next ‘token’ in a sequence (of words) [4]. From this apparently modest objective function, increasingly sophisticated capabilities emerged as models scaled in parameter count, training data, and computer resources [5]. Reasoning, summarisation, coding assistance, translation, and scientific synthesis have not been programmed explicitly, they appeared as emergent properties of scale.
The scientific beauty of both systems lies in the disproportionate differences between the mechanisms and their outcomes. GLP-1 signalling modifies caloric behaviour through subtle hormonal modulation; LLMs generate cognitively persuasive outputs through probabilistic token prediction. In both cases, solutions to immensely complexity problems emerge through the exploitation of comparatively simplistic underlying rules.
Importantly, both technologies rapidly exceeded their original design goals. GLP-1 receptor agonists were initially developed for type 2 diabetes mellitus. Yet clinical evidence built up radidly demonstrating benefits extending far beyond simple glycaemic control. Cardiovascular outcome trials have shown reductions in cardiovascular events, including myocardial infarction and stroke [1][6]. Emerging evidence suggests additional therapeutic benefits in chronic kidney disease, fatty liver disease, obstructive sleep apnoea, addiction, neuroinflammation, and neurodegenerative disorders [7].
This expansion reflects the wider physiological role of GLP-1 biology throughout the body. The drugs appear not merely metabolic regulators but systemic modulators of inflammatory, behavioural, and vascular processes. In some patients, reductions in compulsive behaviours, including alcohol consumption and binge eating, suggest effects on reward circuitry itself [7].
LLMs have undergone a similar trajectory. Initially conceived as natural language processing systems, they rapidly evolved into general-purpose cognitive tools. Their applications now span medical decision support, software engineering, legal drafting, scientific discovery, personalised tutoring, and research acceleration [8][9]. In medicine alone, LLMs are being explored for radiology reporting, clinical summarisation, patient triage, medical education, and biomedical literature synthesis [8].
Crucially, neither GLP-1 therapies nor LLMs remain confined to their founding domains. Both have become infrastructural technologies, systems that alter broader patterns of human behaviour and institutional organisation. GLP-1 drugs are reshaping public discussions about obesity, self-control, and chronic disease management; some of societies greatest medical challenges. LLMs are transforming assumptions about expertise, cognition, authorship, and labour itself.
In both cases, the associated benefits carry substantial environmental and industrial costs. The mythology we often build around elegant technology tends to obscure the enormous physical infrastructures required to sustain it.
GLP-1 drugs depend upon sophisticated pharmaceutical manufacturing systems involving peptide synthesis, sterile injectable delivery devices, refrigeration logistics, and global supply chains [10]. Their rapid adoption has already produced shortages, access disparities, and concerns regarding healthcare sustainability [3]. Chronic long-term administration raises additional questions regarding pharmaceutical industrialisation on a population scale. I won’t even begin to address the issue access only being available to those who can pay.
The environmental burden of LLMs is even more visible. Training frontier-scale models requires enormous computational resources, specialised graphics processing units (GPUs), large-scale data centres, and substantial electricity and water consumption [11]. Carbon emissions associated with AI training and inference have become major concerns as models continue to scale [12]. Rare-earth mineral extraction, semiconductor fabrication, and energy-intensive cooling infrastructures further increase ecological costs.
Although this article is playful, the parallel is revealing. Both technologies promise profound human benefit while simultaneously increasing industrial dependency and planetary strain. They represent a modern technological paradox: solutions to human limitations that intensify pressure on shaky environmental systems.
Despite these similarities, the long-term trajectories of GLP-1 drugs and LLMs diverge fundamentally as one is biologically bounded while the other is informationally scalable.
GLP-1 therapeutics, however transformative, remain constrained by human physiology. Their benefits ultimately encounter ceilings imposed by receptor biology, adverse effects, tolerability, and metabolic adaptation. Even increasingly sophisticated multi-agonist compounds remain tied to finite therapeutic domains [1]. Human metabolism can be optimised only within certain biological parameters.
LLMs face no comparable intrinsic biological boundary. Their scaling properties suggest continuing performance gains through increases in data, compute, multimodal integration, memory architectures, and autonomous tool use [5]. Unlike pharmaceuticals, software systems are substrate-independent. They can replicate globally at near-zero marginal cost, integrate recursively into research systems, and now they are accelerating their own development.
This distinction may prove historically decisive. GLP-1 drugs will, for a time, be one of the most important pharmaceutical classes ever developed. LLMs, by contrast, may evolve into foundational civilisational infrastructure analogous to electricity, literacy, or the internet itself.
The philosophical implications are equally profound. GLP-1 drugs challenge deeply embedded cultural narratives regarding discipline, willpower, and obesity. By demonstrating that appetite and compulsive eating can be pharmacologically modified, they weaken simplistic moral frameworks surrounding body weight and self-control.
LLMs similarly destabilise assumptions about uniquely human cognition. If language generation, summarisation, pattern recognition, and increasingly sophisticated reasoning can emerge from scalable statistical systems, then aspects of intelligence once considered intrinsically human may instead reflect computationally reproducible processes. Their use also results in the loss of the ‘processing’ abilities of the users [13]. Both technologies therefore provoke discomfort because they blur boundaries between biology and engineering, agency and mechanism, personhood and systems design.
In conclusion, GLP-1 therapies are maturing into highly effective but biologically constrained medical tools. In contrast, LLMs continue expanding into increasingly general cognitive infrastructure with few perceivable theoretical limits. One revolution optimises the human organism. According to a recent publication, the other may fundamentally transform the informational substrate of civilisation itself [14].
References

Get our latest news and publications
Sign up to our news letterResources
Social


Contact us
Address
Niche Science & Technology
Unit 26 Falstaff House
Bardolph Road
Richmond TW9 2LH
United Kingdom
