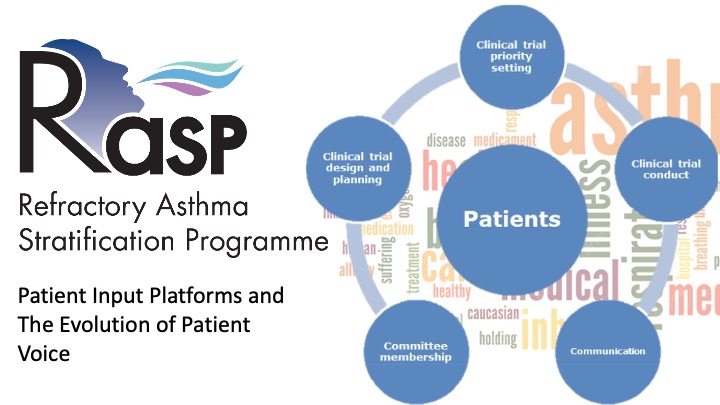
As we stand at the threshold of launching the Medical Research Council’s Refractory Asthma Stratification Programme (RASP‑UK), we do so with a sense of both scientific ambition and cultural transformation. Severe asthma remains one of the most challenging respiratory conditions to manage, characterised by heterogeneity, unpredictable exacerbations, and a heavy burden of treatment—particularly corticosteroids—on patients’ daily lives. The RASP‑UK initiative seeks to address these challenges through biomarker‑driven stratification and innovative clinical study design. Yet, what distinguishes this programme from many that came before it is not only its scientific sophistication, but its commitment to embedding the patient voice at the heart of the research process.
This commitment is not merely symbolic. It reflects a growing recognition across the research community that patients bring forms of expertise that clinicians and scientists cannot replicate: the lived experience of navigating severe asthma, its comorbidities, and the healthcare systems designed to treat it. Over the past two decades, the literature has increasingly demonstrated that patient involvement enhances the relevance, feasibility, and impact of clinical research [1–7]. However, despite this evidence, patient involvement has too often been limited to late‑stage consultation or participation as research subjects rather than as partners in shaping research questions, study design, and dissemination [8]. RASP‑UK offers an opportunity to change that trajectory.
A New Model of Partnership
Our partnership with Asthma UK is central to this vision. Asthma UK brings not only organisational expertise but access to a community of individuals living with severe asthma who are motivated to contribute to research that directly affects their lives. Their involvement began even before the MRC funding decision, with patients helping to shape the programme’s central research question. This early engagement aligns with best practice recommendations that emphasise the importance of involving patients at the inception of research, when their insights can meaningfully influence study direction [8–10].
One of the clearest examples of this influence is the identification of oral corticosteroid burden as a priority outcome. Patients consistently described the profound physical and psychological toll of long‑term steroid use—weight gain, mood disturbance, sleep disruption, and increased infection risk. While clinicians have long recognised these side effects, hearing directly from patients reframed the issue as a central determinant of quality of life. As a result, reduction in corticosteroid exposure became a key endpoint in RASP‑UK’s Work Strand 1, demonstrating how patient priorities can shape scientific priorities.
This is precisely the kind of impact that patient input platforms (PIPs) were designed to achieve. Evidence from earlier initiatives, including U‑BIOPRED, shows that when patients are engaged early and consistently, they can influence study design, improve the clarity of participant‑facing materials, and enhance recruitment strategies [8]. RASP‑UK builds on these lessons, aiming for deeper and more continuous involvement.
Expected Benefits for Study Design and Conduct
The benefits of patient involvement extend across the research lifecycle. First, patients can help ensure that study materials, protocols, consent forms, information sheets, are accessible and meaningful. Research from U‑BIOPRED demonstrated that scientific language often obscures rather than clarifies, and that patient review can significantly improve comprehension for prospective participants [8]. In RASP‑UK, the PIP will review all participant‑facing documents, ensuring that they reflect the realities of living with severe asthma and communicate risks and procedures in a way that supports informed decision‑making. Thanks to our involvement with Asthma UK, they are already involved in preliminary study design and protocol development.
Second, patient involvement is expected to enhance recruitment and retention, two of the most persistent challenges in severe asthma research. In U‑BIOPRED, patient‑generated materials, like personal accounts of bronchoscopy, helped demystify procedures and reduce anxiety among potential participants. Although formal impact metrics were not collected, investigators reported that these contributions were valuable in addressing recruitment barriers. RASP‑UK anticipates similar benefits, particularly in studies involving invasive procedures or intensive biomarker profiling.
Third, patients can provide critical insight into the feasibility and acceptability of study procedures. Severe asthma is a condition marked by fluctuating symptoms, frequent hospitalisations, and substantial treatment burden. Patients are uniquely positioned to identify aspects of study design that may be impractical or overly burdensome. Their input can help refine visit schedules, reduce unnecessary procedures, and ensure that the research respects participants’ lived realities. This aligns with broader evidence showing that patient involvement improves study feasibility and reduces protocol amendments [3][4][7].
Enhancing Scientific Relevance and Impact
Beyond operational benefits, patient involvement strengthens the scientific relevance of the research. Their perspectives can illuminate aspects of disease experience that may not be captured by traditional clinical endpoints. For example, in RASP‑UK so far, patients emphasised the importance of day‑to‑day symptom variability, fatigue, and the cumulative burden of steroid side effects, factors that may not be fully reflected in exacerbation rates or lung function measures alone. Incorporating these insights can lead to more holistic outcome measures and a richer understanding of treatment impact.
Involving patients in the interpretation and dissemination of findings ensures that research outputs are meaningful to the communities they aim to serve. U‑BIOPRED demonstrated the value of patient co‑authorship and lay summaries in broadening the reach and accessibility of scientific publications [8]. RASP‑UK intends to extend such practices and involvement, recognising that patients are powerful advocates who can communicate research findings through social media, patient networks, and public forums.
Cultural Transformation and Long‑Term Legacy
Perhaps the most profound impact of patient involvement is cultural. As with U‑BIOPRED, our clinical team initially expressed concern that patients might struggle to engage with complex scientific concepts. Over time, these assumptions were challenged, and researchers came to appreciate the value of lay interpretation and the importance of communicating science in accessible terms. This shift in mindset is essential for building a more inclusive and responsive research environment.
RASP‑UK has the opportunity to accelerate this cultural transformation. By embedding patient involvement from the outset, the programme signals that patient expertise is not peripheral but central to the research endeavour. This approach aligns with emerging standards for public involvement, which emphasise inclusivity, collaboration, communication, and impact. Although these standards were introduced after RASP‑UK was conceived, the programme is well positioned to exemplify their principles.
Conclusion
As we embark on the RASP‑UK initiative, we do so with a conviction that patient involvement is not merely an ethical imperative but a scientific one. By partnering with Asthma UK and engaging individuals living with severe asthma as co‑creators of knowledge, we expect to design studies that are more relevant, feasible, and impactful. We anticipate improvements in recruitment, enhanced clarity of study materials, and the development of outcomes that reflect what truly matters to patients. Most importantly, we foresee a research culture that values and integrates patient expertise, setting a precedent for future respiratory research.
RASP‑UK represents not only a scientific opportunity but a chance to redefine how we conduct clinical research. By listening to patients, before the first participant is enrolled, we lay the foundation for discoveries that are not only scientifically robust but deeply meaningful to those who stand to benefit most.
References
- Chalmers I. BMJ. 1995;310:1315–8.
- Baggott R. Healthy democracy: the future of involvement in health and social care. Health Expect. 2008 Jun;11(2):202–3.
- Domecq JP, et al. BMC Health Serv Res. 2014;14:89.
- Boote J, Wong R, Booth A. Health Expect. 2015.
- Barber R, et al. Health Expect. 2012;15:229–41.
- Edelman N, Barron D. Evaluation of public involvement in research: time for a major re-think? J Health Serv Res Policy. 2016 Jul;21(3):209-11.
- Brett J, et al. Health Expect. 2014;17:637–50.
- Supple D, et al. Res Involv Engagem. 2015;1:5.
- Caron‑Flinterman JF, et al. Health Expect. 2005;8:253–63.
- Slade M, et al. BMC Health Serv Res. 2010;10:323.