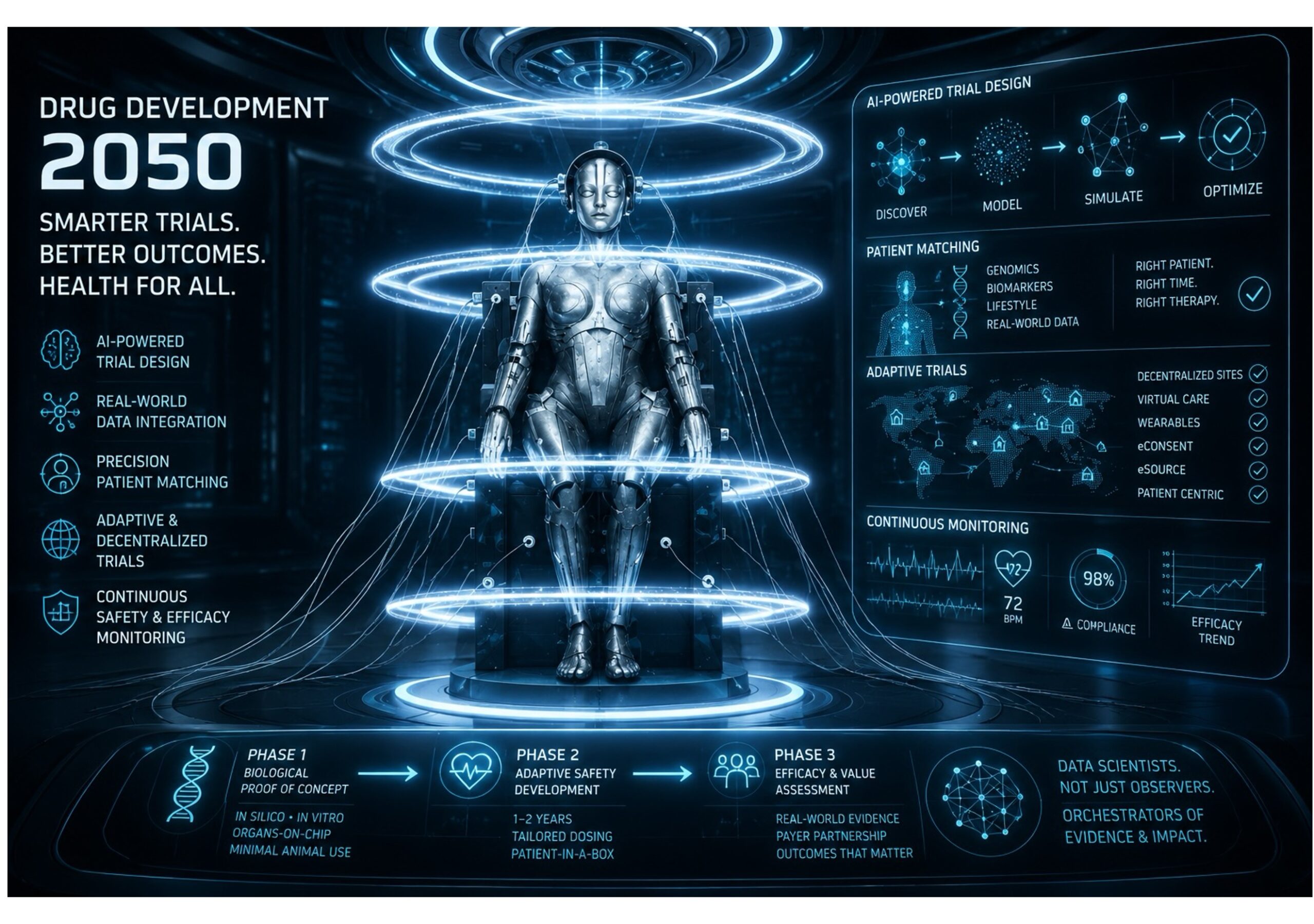
In September 2022, more than 200 delegates attending the 18th Annual Conference of the Pharmaceutical Contract Management Group (PCMG) in Krakow participated in a forward-looking workshop exploring what clinical drug development might resemble in 2050 [1]. The attendees represented a collective experience estimated at more than 2500 years across pharmaceutical development, outsourcing, clinical operations and regulatory science. Rather than presenting a formal predictive model, the workshop used structured discussion questions and consensus-based debate to derive expert opinion on future trends in clinical research. The resulting article, published in 2023, captured a striking vision of a data-driven, AI-enabled and highly adaptive future for drug development [1].
The workshop discussions focused on four central questions: who will lead the pharmaceutical industry in 2050; how wearable technologies and implanted biosensors will influence patient selection; how artificial intelligence (AI) will design and manage clinical trials; and how the role of the Clinical Research Associate (CRA) may evolve [1]. The consensus view emerging from the discussions was clear: the future clinical trial ecosystem will be dominated by data science.
The article, published today and authored by Niche’s Managing Director, Dr Tim Hardman (me), argues that the historical pharmaceutical model built around sequential clinical trial phases and heavily manual oversight may become unsustainable in the face of exploding data complexity [1]. Current drug development already generates unprecedented volumes of structured and unstructured information from genomics, biomarkers, electronic health records and real-world evidence sources [2][3][4][5]. By 2050, delegates envisioned a world in which wearable sensors, implantable ‘health chips’, smart pills and continuously connected monitoring systems routinely collect physiological and behavioural data from entire populations [1][6]. Rather than episodic participation in trials, individuals may contribute longitudinal health information continuously.
This concept aligns with earlier literature describing the emergence of the Internet of Things in healthcare and pharmaceutical development [6]. The workshop participants predicted that implanted biosensors and wearable technologies would transform not only disease monitoring but also drug delivery itself. Responsive delivery systems capable of automatically adjusting dosing according to physiological changes were considered likely to replace conventional fixed-dose approaches [1]. In diseases such as diabetes, this future would involve automated sensing and drug administration systems that continuously optimize therapy without direct patient intervention.
A major theme throughout the workshop was the growing influence of AI. Delegates proposed that AI systems would increasingly optimize protocol design using historical trial data from registries such as ClinicalTrials.gov [1]. Machine learning algorithms could reduce protocol amendments, improve endpoint selection and identify high-performing research centres and suitable participants more efficiently than traditional recruitment approaches [7][8]. The broader scientific literature before 2022 already supported this direction, particularly in radiology, diagnostics and disease prediction, where AI systems demonstrated expanding clinical utility [9][10][11].
The workshop also anticipated the rise of synthetic and simulated clinical cohorts. Using integrated real-world patient data and advanced modelling techniques, AI-driven simulations may eventually reduce dependence on placebo groups and accelerate dose optimization and safety profiling [1]. Such predictions reflect broader concerns regarding the inefficiency of traditional pharmaceutical development. Drug development timelines frequently exceed 7–10 years, with attrition rates remaining extremely high despite decades of regulatory modernisation [12].
One of the most provocative proposals arising from the workshop was a reimagined regulatory framework. Delegates predicted that the traditional sequential Phase I–III structure could evolve into a continuous, adaptive registration pathway [1]. In this model, early development would focus on biological proof-of-concept using engineered human tissues and computational models, potentially reducing reliance on animal testing. Once preliminary safety is established, therapies would enter an ongoing adaptive clinical development programme conducted largely in patients and continuously updated using real-time data.
Importantly, regulators themselves were expected to become increasingly integrated into the development process through shared digital platforms and real-time oversight [1]. This vision echoes earlier regulatory discussions from the European Medicines Agency and FDA regarding expedited pathways and adaptive licensing frameworks [13]. Delegates suggested that globally harmonized oversight could dramatically reduce administrative delays associated with protocol amendments and multi-country submissions.
The future role of clinical professionals also emerged as a major discussion point. Participants believed that traditional CRA roles centred on on-site monitoring and source verification would largely disappear due to automation and centralized digital oversight [1]. Clinical trials might instead occur within “patient-in-a-box” environments involving virtual clinics, microsites or even patients’ homes. The future workforce would therefore require expertise in informatics, algorithm management and data interpretation rather than conventional site management.
Beyond operational transformation, the workshop highlighted broader societal implications. Delegates emphasized that healthcare expenditure is becoming increasingly unsustainable, particularly as ageing populations drive rising prevalence of chronic diseases [14][15]. The future reimbursement landscape may therefore depend on shared-risk agreements, outcomes-based payment models and patient participation in data-sharing ecosystems [1]. In this vision, individuals contributing their health data to development programmes might receive reduced treatment costs or preferential access to therapies.
The article also predicts that medicine itself will become increasingly individualised. Advances in genomics, biomarker science and cellular therapies are expected to shift treatment away from generalized symptom management towards dynamic, patient-specific intervention [1]. Technologies such as CRISPR, targeted protein degradation and immuno-oncology already suggested this trajectory before 2022 [1]. The workshop participants argued that diseases may eventually be reclassified according to molecular and mechanistic signatures rather than traditional symptom-based descriptions.
Ultimately, the article presents a future in which clinical drug development becomes less about isolated clinical trials and more about continuous, integrated learning systems driven by data. By 2050, pharmaceutical innovation may depend less on conventional organizational structures and more on those capable of controlling and interpreting vast health datasets. The delegates concluded that the defining professional of future clinical development will not primarily be the clinician or pharmacologist, but the data scientist [1].
References
- Hardman TC, et al. The future of clinical trials and drug development: 2050. Drugs Context. 2023;12:2023-2-2.
- Tufts Center for the Study of Drug Development. Impact report: analysis and insight into critical drug development issues. Vol 1, No 1. Jan/Feb 2021.
- Marsolo KA, Richesson R, Hammond WE, Smerek M, Curti L. Common real-world data sources. Rethinking Clinical Trials.
- Tufts Center for the Study of Drug Development. Tufts-eClinical solutions, data strategies and transformation study.
- Assessing fitness for use of real-world data sources: data provenance. Rethinking Clinical Trials.
- Singh M, Sachan S, Singh A, Singh KK. Internet of Things in pharma industry: possibilities and challenges. In: Balas VE, Solanki VK, Kumar R, editors. Emergence of Pharmaceutical Industry Growth with Industrial IoT Approach. London: Academic Press; 2020.
- Toddenroth D, Sivagnanasundaram J, Prokosch HU, Ganslandt T. Concept and implementation of a study dashboard module for continuous monitoring of trial recruitment and documentation. J Biomed Inform. 2016;64:222-231.
- Hird N, Ghosh S, Kitano H. Digital health revolution: perfect storm or perfect opportunity for pharmaceutical R&D? Drug Discov Today. 2016;21(6):900-911.
- Nichols JA, Herbert Chan HW, Baker MAB. Machine learning: applications of artificial intelligence to imaging and diagnosis. Biophys Rev. 2019;11:111-118.
- Hosny A, Parmar C, Quackenbush J, Schwartz LH, Aerts HJWL. Artificial intelligence in radiology. Nat Rev Cancer. 2018;18(8):500-510.
- Yuan Q, Zhang H, Deng T, et al. Role of artificial intelligence in kidney disease. Int J Med Sci. 2020;17(7):970-984.
- Wouters OJ, McKee M, Luyten J. Estimated research and development investment needed to bring a new medicine to market, 2009-2018. JAMA. 2020;323(9):844-853.
- US FDA Center for Drug Evaluation and Research. Expedited programs for serious conditions – drugs and biologics. 2014.
- McNicoll G. World population ageing 1950-2050. Popul Dev Rev. 2002;28(4):814-815.
- Healthy Aging Team. The top 10 most common chronic diseases for older adults. National Council on Aging.